
The truth is that buying weed online using the internet is now reasonably straightforward (thanks to Bitcoin and the Dark Web) and there are professional, trusted vendors just waiting to serve your needs as a customer.
I’m going to show you exactly how to do it right here on Medicine Man, in this step by step guide. They are a UK collective that has been running for some years now. Cannabis only with deliveries reaching Germany, Ireland and France as well as the UK.
Make sure you read the news section at Medicine Man UK and check out the forum for any info you may need before emailing them directly.
With recreational weed is legal in California it’s only a matter of time before our archaic and uncaring laws catch up.
The police don’t have the resources to stop crime going up all over the country, so you can pretty much guarantee they do not have the resources to be pursuing Joe Smith ordering an eighth of weed on the web.
It’s just not going to happen. I have personally used this method literally hundreds of times and the orders always come through.
According to one London postman speaking to the BBC:
“I’ve spent 14 years as a postman in uniform and I have never seen a drug dog.”
Another postie confirms:
“If it’s got a stamp on it, you post it. We don’t have drug dogs to smell every parcel. We don’t have the resources to X-ray every parcel. We just have to deliver it and take the risk. Our job is to deliver it safely to the customer.”

You can order small amounts of cannabis with absolute confidence. You are entitled to use this and all plants. It’s almost legal now. It will arrive in an innocent looking packet, double vacuum sealed.
It’s a simple process, which is laid out below.
If you don’t want to mess about with Tor Medicine Man now have a normal link to access their service.
You can do this on a mobile phone. On the iPhone ensure you download Ornet instead of Tor. This is by far the best Tor equivalent for iPhone.

1. Download the Exodus Wallet.
Exodus is one of the best wallets that you can use. It is secure and very easy to navigate.
Check out their reviews if you are unsure.
Exodus also has a super simple way to buy Bitcoin which is built into the wallet (using Ramp) making purchasing small amounts of crypto straightforward.
Download here for Android.
Or here for the iPhone.
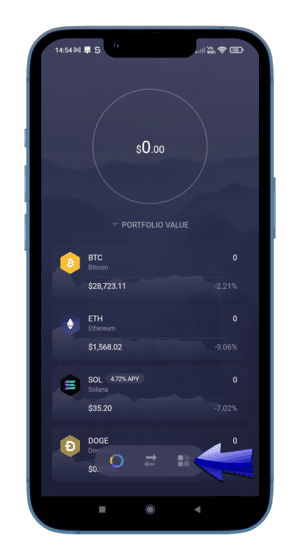
2. Buy Bitcoin.
Once your wallet is installed press the dashboard button on the right hand side of the navigation area.
This is the little icon with the four squares which the blue arrow is pointing to as shown.
Obviously you can buy Bitcoin from anywhere, this is just one vendor. Check inside the Medicine Man forum for other buying options.

3. Click ‘Buy Crypto’.
Now simply press the ‘Buy Crypto’ button which the blue arrow is pointing to.
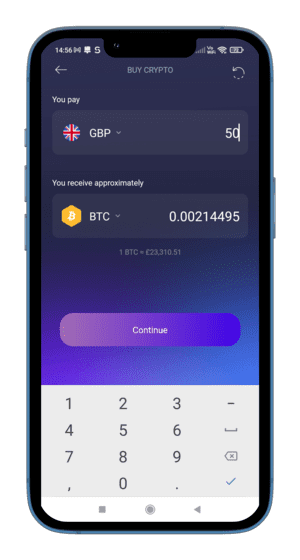
4. Select amount and buy.
Select the amount that you want to buy. I would recommend £45 or £50.
If you buy a small amount (ie less than $100) then you may not have to go through any verification process and you can buy Bitcoin using your card quickly.
Your BTC wallet address on Exodus is automatically included in the checkout, so you don’t need to tell them where to send it to.
Go through the purchase process and your Bitcoin will appear in your Exodus wallet once complete.
This will take a few minutes.

5. Download Tor Browser.
Now Download Tor (Android) or if you are on iPhone download Ornet.
Install it and then open it.
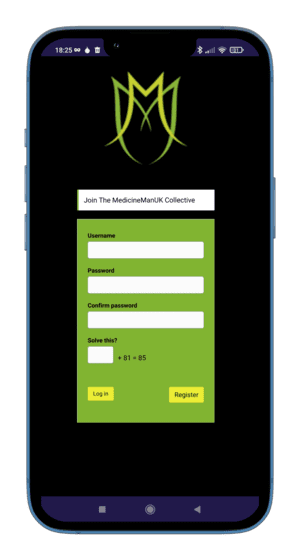
6. Create Account on Medicine Man.
Sign up to Medicine Man using this link. The whole process should take just a few seconds.
Make sure you can remember your password and username, or write it down.

7. Go to your wallet section.
Go to the wallet area.
Use the menu at the top right as shown to go to ‘My Account’ and then select the ‘My Wallet’ link.
Input how much you want to send to Medicine Man (£45 will more than cover you for an 1/8, including shipping).
It’s better to send slightly more, then you wont have to repeat the process.
Bear in mind that each time you send BTC a small transaction fee is paid.

8. Proceed to checkout.
Once you have selected the amount go to checkout.
Obviously you haven’t selected any product yet, (don’t panic) just press the checkout button and you will be taken to the next screen.
You have to top up your wallet before ordering.
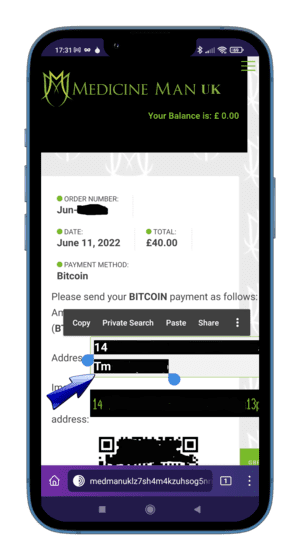
9. Get wallet address.
Now copy the full Bitcoin address as shown by the blue arrow. This is your Bitcoin address for this top up.
Some if it has been blacked out on this image.
Be very careful here as if you get this wrong then your Bitcoin will not go where you want it to.
Make sure you have copied the full address correctly.
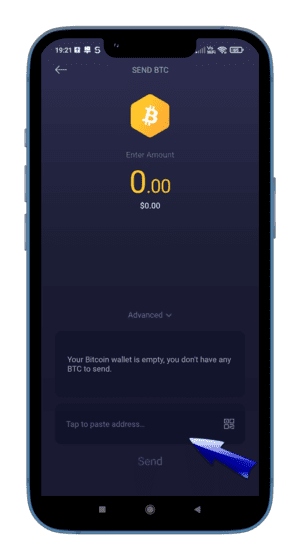
10. Send from Exodus.
Now go back to your Exodus wallet and whilst in the Bitcoin section click on the upward pointing arrow icon shown below to get the ‘Send BTC’ screen.
Paste in your wallet address in the area shown by the blue arrow and input the amount to send.
Once sent it will take a few minutes to appear in your Medicine Man wallet area.
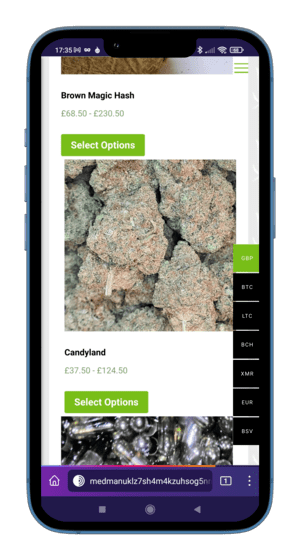
11. Go shopping.
You are now all set to buy some weed! I’m sure you don’t need a guide to putting products in your basket. You got this.
Find yourself a nice looking bit of bud and add it.
You might want to check out the very useful review section which is shown under a tab for all products.
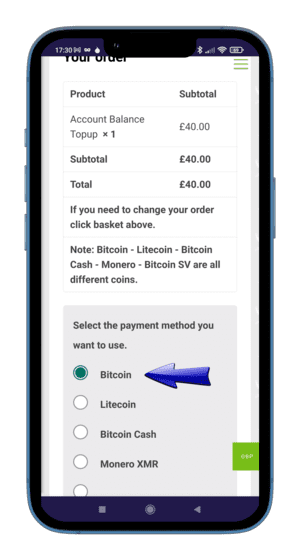
12. Checkout your item.
Checkout.
Here you’ll need to select which cryptocurrency you are using.
Select Bitcoin as shown.

13. Select shipping options.
Select the required shipping option.
This is pretty self explanatory.

14. Final stage.
Enter your mailing address and complete the order.
Do not use fake names and don’t use any special characters like commas, just the name and address.
Now await delivery!
- Amnesia Haze
- Banana Pie
- Blackberry Fire
- Blue Cheese
- Blueberry Muffin
- Bruce Banner
- Casey Jones
- Cherry Pie
- Clementine
- Critical Silver Haze
- Durban Poison
- Dutch Passion Haze
- Dutch Treat
- Forbidden Fruit
- Gas
- Gelato #33
- Gelato Cookies
- Gold Seal Hash
- Grapefruit Diesel
- Ice Cream Man
- Jack Herer
- Kandy Kush
- Lemon Cake
- Lemon Cake Keif
- Lemon OG Kush
- Mango Sherbet
- Medicated Nerdz Ropes
- Moonrocks – Mango
- Moonrocks – Watermelon OG
- Moonrocks – Stardawg
- Moroccan Hash
- New York Diesel
- Papaya
- Pearl Scout Cookies
- Pineapple Express
- Pink Lady Kush
- Pre-roll Cannabis Packs
- Purple Punch
- Rick Simpson Oil
- Rockstar
- Runtz
- Skywalker OG
- Stardawg
- Sundae Driver
- Super Silver Haze
- Tangerine
- Tuna Kush
- Vape – Grape Ape
- Vape – Pineapple Express
- Vape – Strawberry Cough
- Zkittlez
Important note: If you’re looking to get hold of cannabis oil for medical purposes, first speak to these guys, who really know their cannabis oil science.
Other CBD related options:
CBD buds are being sold openly in the UK now and contain very low levels of THC but do contain other beneficial cannabinoids such as CBD which can reduce pain, inflammation and anxiety as well as having other positive effects.
These buds looks just the same as cannabis buds and provide the stress and pain relief of cannabis without the psychedelic brain effects that can occur with THC.
See this page for more information about buying CBD oil. If you want to take care of things yourself, then see this page about cannabis seeds.
If you are in Canada you have the luxury of using a clearnet online dispensary.
Frequently Asked Questions About Buying Cannabis
Where can you buy cannabis online?
How much does weed cost online?
Why should you buy weed online?
Is it easy to buy cannabis online in the uk?
Does everyone use Bitcoin to purchase cannabis online?
Is it more expensive to purchase weed online?
How long does weed delivery take?
Can you buy 10 10 vapes in UK?
Where to buy medicinal cannabis in the UK?
Can you buy cannabis concentrates online in the UK?
Where can you buy weed online in the UK?
There are a growing number of places to buy weed online in the UK. However, if you are looking for an extensive catalogue of weed and rapid delivery then one of the best places to check out is Medicine Man.
They run a shop which can be accessed by using the Tor browser online. After several years they have built up a reputation for consistency and quality.
How much does weed cost online?
Medicine Man have recently started selling some of their deals for as low as £27 for an eighth. That is not for low quality weed either, some very respectable Blue Dream can be bought for this price. Ounces go for an average of £210.
Many of the shops that you find online are asking extortionate amounts of money for weed. Most of these sites are total scams.
It’s actually incredibly easy to set up an online cannabis store that looks completely real. That is why it is good practice to avoid the clear net (ie normal websites) when buying weed online and stick to established websites on the dark web.
Why should you buy weed online?
Buying online these days makes a lot more sense for several reasons.
Choice is one great plus. Where else are you going to find a choice of 40 different strains to buy without traveling to a licensed medical cannabis dispensary/weed shop in the US or a coffee shop in Amsterdam?
If you know you like ‘Sativa’ effects or ‘Indica’ effects then you can choose a high quality strain with a potency that fits your personal preferences.
Reliability is another good reason. Vendors live and die by their reviews. Just like on Ebay. So it has become very difficult to buy bad cannabis if you allow yourself to be guided by reviews on an established dark web website.
The onus is on the seller to make sure that they have the best possible products for sale online.
Then there is convenience. Obviously you don’t have to spend any time travelling around to meet your man (or lady) so that time saved is an added bonus. Only a short walk to your letterbox is required once you have ordered. See this video for a buying demonstration.
Is it easy to buy weed online in the uk?
It is very easy to buy weed using the Internet in the UK. In most cases the longest part of the process is actually getting hold of the Bitcoin in the first place. Once you have done this and actually have the Bitcoin in your possession, things are normally pretty fast.
It’s then just a case of getting your Bitcoin onto the vendors’s website and choosing the strain that you want to order, and ordering it.
For example it would certainly be possible to place an order on somewhere like Medicine Man in less than five minutes. The first time there is obviously a small learning curve to overcome.
Does everyone use Bitcoin to purchase weed online?
There are websites online that accept credit cards for weed, but a very high percentage of these websites are scam websites set up by people to take advantage of those who do not know better.
The Internet makes it very difficult to carry out any kind of a check on a website like this, so whatever you do don’t go buying weed from some random website, just because it appears in Google does not mean that it is can be trusted.
It is for this reason, as well as privacy, that most online cannabis stores operate on the darknet using Bitcoin and other cryptocurrencies. Buying weed directly with a credit or debit card adds extra risk to the whole process and should be avoided.
Is it more expensive to purchase weed online?
It all depends who you know. Online prices are normally lower than prices on the street. Having said that if you know the right people cannabis can get very cheap, especially if you know a friendly grower.
The average price for an ounce of weed on Medicine Man is £220 with eighths for sale from £27 plus delivery. Most street dealers want £35 or more for this quantity of high quality cannabis.
How long does weed delivery take?
You hear a lot about ‘NDD’ these days, or, next day delivery. In most cases this is a little bit optimistic but if you place an order on a Monday with a professional vendor then you stand a very good chance of getting it by the Wednesday in the UK.
If you place on order on Wednesday then expecting it to arrive by Friday is realistic. You get the picture.
Not everybody has the distribution infrastructure of Amazon, a couple of days is pretty good when you think about it.
These guys have specific delivery schedules which you can find on their website.
Can you buy 10/10 Vapes in the UK?
Medicine Man do sell the famous 10/10 vapes that you will have been seeing around.
These are American imports that really do the trick. Stealth is off the scale and after a couple of goes on one of these things you definitely feel the effects.
From personal experience I would say this is a much stronger experience than it is vaping normal flower. These are pure cannabinoid extractions with very specific tastes and effects.
I was very impressed indeed and will be getting some more more of these. They are ideal for travel or places where it is just not cool to spark up a dooby.
Where to buy medical cannabis in the UK?
‘Medical’ cannabis is a little bit of a misnomer, there are some strains that contain more CBD which have been specifically bred to be this way, but THC is also medically beneficial so one cannot say that only CBD rich strains are medical.
Many THC heavy strains contain small amounts of CBD and other cannabinoids and most hashes are high in CBD content.
Websites like Medicine Man sell a number of products that could well be classed as ‘Medical’ cannabis.
If you have several thousand pounds a month spare you can currently use a private cannabis clinic to get a prescription (if you have an accepted medical condition).
Alternatively (as it is the only option for many) you can buy highly effective cannabis from the dark web, have a good look at reviews, many of which are from long term ‘medical’ cannabis users.
Can you buy cannabis concentrates online in the UK?
Medicine Man are currently showing ‘Stardawg Concentrate’ shatter for sale at £55 per gram.
They also have Whitefire OG at £50 per gram and Rick Simpson Oil which has been produced using ‘closed loop extraction’ at £70 per 2ml sealed in a syringe.
A contained ‘Closed Loop’ system makes the risk of contamination from solvent virtually non-existent when producing cannabis oil.

Yo, I have had nothing but good times with medicine man. They are a professional outfit with some proper chong. Highly recommended.
NDD most of the time.
Came after a coople of days. Depends when you order.
Good gear though. Reliable.
Been using these guys several months. Always gets through to the EU 🙂
Cherry Pie is the shit!!!!
Do they sell soft black hash, for obvious reasons the supply chain was restricted last 20 years . Very few and far between I get the option in my town .